Why this topic matters
The purpose of reliable information about KRAS, NRAS and BRAF Tests in Colorectal Cancer is to help a patient recognise relevant symptoms, seek appropriate assessment and avoid unsafe self-treatment.
These tumour markers are not general screening tests. They are used in defined clinical settings, particularly when oncology treatment selection requires them.
Understanding when tumour molecular results may guide systemic treatment requires age, symptom duration, family history, medicines, previous procedures and overall health to be considered together.
What it means and what it does not mean
KRAS, NRAS and BRAF Tests in Colorectal Cancer cannot be confirmed by an internet label.
One symptom, photograph or test result is not a complete diagnosis; conclusions without clinical context and examination may be wrong.
These tumour markers are not general screening tests. They are used in defined clinical settings, particularly when oncology treatment selection requires them. Similar symptoms can occur in other colorectal or gastrointestinal conditions, so a cause-based assessment matters.
Who should consider assessment
A diagnostic test is useful only when its result can answer a defined clinical question or change management. Reports must be interpreted with symptoms, examination and other investigations.
Review is reasonable when symptoms continue for several weeks, interrupt normal activity, repeatedly return or fail to improve after an appropriate first treatment.
Tell the clinician about family history, previous polyps or cancer, inflammatory bowel disease, blood thinners, diabetes and immune problems because these details can change the pathway.
What to record before a consultation
Write down when the symptom started, how often it occurs, what makes it better or worse and the pattern of stool or bleeding.
Bring previous prescriptions, endoscopy, biopsy, CT or MRI, blood tests and operation notes rather than relying on memory.
Record weight trend, appetite, fever, pain, discharge, bowel frequency and relevant cancers in close relatives so important clues are not missed.
How diagnosis is approached
Before testing, the clinician reviews the reason for the test, preparation, kidney or allergy risk, medicines, previous reports and the consequence of a positive or negative result.
A focused abdominal, rectal or anal examination may follow the history and should be performed with explanation, consent and privacy.
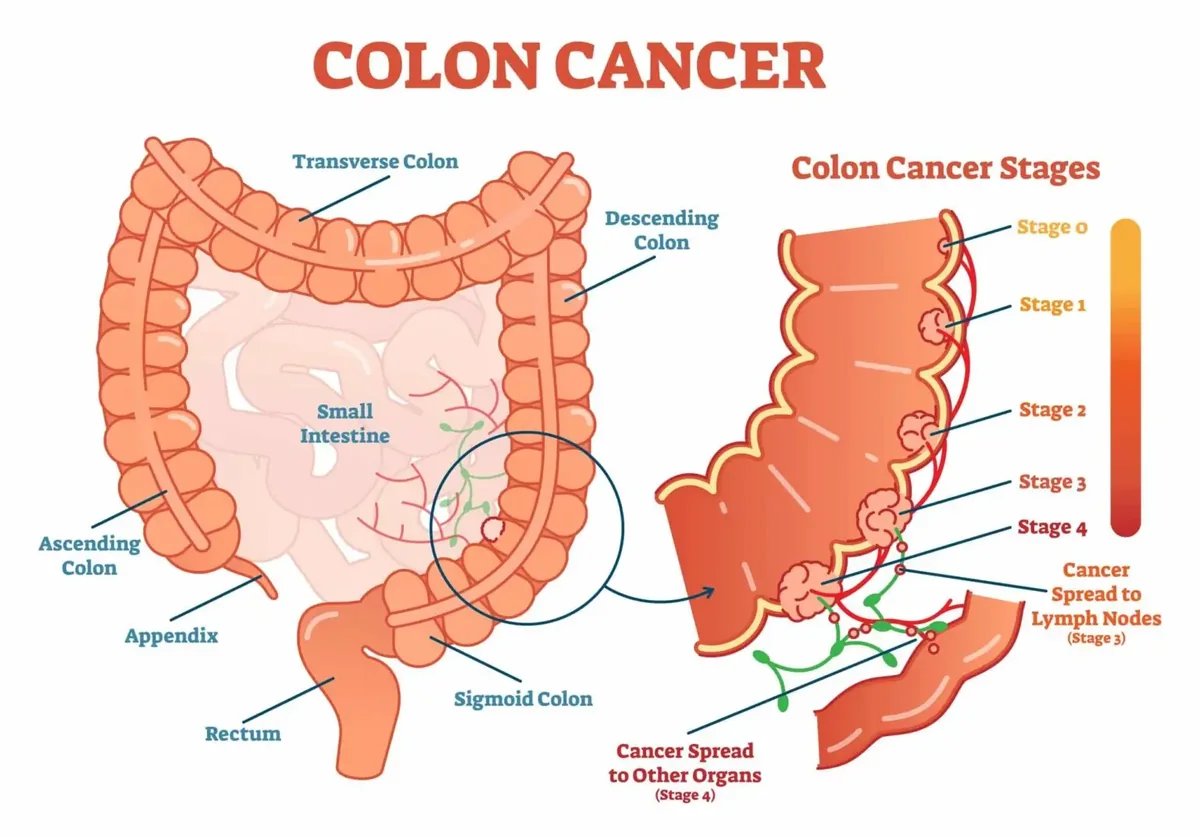
A test should answer a defined question: confirm the diagnosis, assess severity, map anatomy, establish stage or change treatment planning.
How to interpret reports
The impression section of a report matters, but image quality, specimen adequacy, timing and agreement with clinical findings also need review.
A normal result does not exclude every disease, and an abnormal result does not automatically mean cancer or an operation.
When results about when tumour molecular results may guide systemic treatment disagree, pathology review, repeat imaging, endoscopy or multidisciplinary discussion may be appropriate.
Non-operative care
No single report should be used in isolation to promise or exclude cancer. Discordant results may need pathology review, repeat imaging, colonoscopy or multidisciplinary discussion.
Depending on the confirmed diagnosis and severity, care may include diet, fibre, hydration, bowel-habit measures, topical treatment or medicines.
Pregnancy, kidney or heart disease, allergy and blood-thinning medicine can alter safety; do not stop a prescribed medicine without advice from its prescriber.
When a procedure or operation is considered
A procedure is selected according to anatomy, disease extent, expected benefit, alternatives and risk rather than its popularity or name.
These tumour markers are not general screening tests. They are used in defined clinical settings, particularly when oncology treatment selection requires them. A procedure may be reasonable in a selected patient, but the same operation is not right for everyone.
Before consent, discuss relevant issues such as anaesthesia, bleeding, infection, recurrence, bowel function, continence, a possible stoma and recovery.
Benefits, limitations and uncertainty
A realistic treatment goal should describe a specific outcome such as control of pain, bleeding, infection, obstruction, prolapse or cancer.
No medicine or operation can honestly guarantee a 100 percent cure or a recurrence-free result.
Expected benefit must be balanced with short-term complications, long-term function, work and family responsibilities and the burden of follow-up.
Recovery and follow-up
A recovery plan should specify pain control, food and fluid, bowel or stoma output, wound care, activity, driving or work and the follow-up date.
If pathology or imaging is pending, know who will review it, when it will be reviewed and how the result will be communicated.
Symptom improvement is encouraging, but follow-up should confirm whether the underlying diagnosis has resolved or needs surveillance.
Urgent warning signs
A test appointment is not emergency care. Heavy bleeding, severe pain, fainting, fever, repeated vomiting or obstruction symptoms need prompt clinical assessment.
Do not wait for an online answer or a routine appointment when emergency symptoms are present.
After a recent operation or procedure, sudden deterioration should prompt contact with the treating team or the nearest emergency department, taking the discharge paper and medicine list.
Practical care decisions in Bangladesh
When choosing a hospital or clinician, review verified qualifications, BMDC registration, relevant training, the diagnostic process, informed consent and the follow-up system.
Unverified Best, Top or guaranteed-cure claims are not substitutes for clinical evidence.
When discussing cost, ask separately about consultation, tests, hospital, anaesthesia, pathology, medicines and follow-up so the plan is transparent.
Questions to ask the care team
Ask how when tumour molecular results may guide systemic treatment will be confirmed and which alternative diagnoses are being considered.
Ask how the recommended test or treatment will change the plan, what realistic benefit is expected and which risks are important for you.
Confirm which symptoms need urgent help, when the next review is due and whether long-term prevention or surveillance is required.
A framework for treatment decisions
Before deciding about KRAS, NRAS and BRAF Tests in Colorectal Cancer, ask how certain the diagnosis is, how severe the current problem is and whether observation or conservative care remains reasonable.
Compare each option in writing by expected benefit, important risks, alternatives, recovery burden and its effect on future treatment choices.
Patient preference matters, but informed preference requires reports, anatomy, uncertainty and realistic outcomes to be explained in language the patient can understand.
When a second opinion may help
A second opinion can clarify planning before major cancer surgery, a permanent stoma, treatment of complex recurrent disease or a decision based on reports that do not agree.
Seeking another opinion does not automatically mean the first clinician is wrong; the new team needs complete reports, actual images, pathology material and previous operation notes when relevant.
Urgent resuscitation, drainage of sepsis or treatment of obstruction should not be dangerously delayed while arranging a non-urgent opinion.
Long-term monitoring and prevention
After the immediate issue related to when tumour molecular results may guide systemic treatment is treated, review bowel habits, nutrition, medicines, family risk and any recommended surveillance.
Follow-up intervals are individual to diagnosis, pathology, procedure and recurrence risk, so an internet schedule cannot safely replace the written plan.
New bleeding, anaemia, weight loss, persistent pain or bowel-habit change should be reassessed rather than automatically attributed to an old diagnosis.
Common misconceptions
A common misconception about KRAS, NRAS and BRAF Tests in Colorectal Cancer is that one test or a modern-sounding procedure provides the final answer for every patient.
Less pain or a smaller incision may be useful outcomes, but they are not the only decision factors when completeness of treatment, safety, function and recurrence are considered.
An online testimonial describes an individual experience; it is not evidence of complication rates, pathology outcomes or what is suitable for your anatomy.
Coordinating multidisciplinary care
Colorectal care may involve gastroenterology, oncology, radiology, pathology, anaesthesia, stoma therapy, nutrition or a pelvic-floor team in addition to the surgeon.
Keep the primary coordinator, pending reports and the next decision point clear in the consultation or discharge plan so important results are not lost between services.
Sharing the current medicine list, allergies, contact details and emergency plan with one responsible family member can improve practical safety during treatment and recovery.
Appointment preparation checklist
Bring photo identification, a current medicine list, allergies, relevant reports and a short symptom timeline to reduce avoidable repetition.
Writing the three main concerns and three questions before the appointment helps keep the discussion focused when time and anxiety make details easy to forget.
An intimate examination may be relevant; patients can ask for an explanation, privacy, consent and the local chaperone policy before it begins.
The role of family and caregivers
If the patient wishes, a trusted person can attend the consultation, take notes and help remember the options without replacing the patient's own preferences.
A caregiver can assist with medicines, hydration, transport, warning-sign monitoring and follow-up organisation while respecting confidentiality and independence.
Before cancer treatment or major surgery, planning work leave, home support, nutrition and emergency transport can reduce practical stress during recovery.
How this article should be used
This page synthesises information from linked clinical authorities and explains it for patient education in a Bangladesh context; it does not reproduce a source article.
Medical information can require revision as evidence and guidance change, so readers should check the page date and the linked source records.
The article is not an emergency service and cannot replace physical examination, a personalised prescription or advice from the clinician responsible for care.
Key takeaways
These tumour markers are not general screening tests. They are used in defined clinical settings, particularly when oncology treatment selection requires them.
A sound sequence is to understand symptoms, confirm the diagnosis, define severity or stage, discuss options and maintain organised follow-up.
This page is for education; an individual diagnosis or prescription requires direct assessment by a suitably qualified clinician.
Frequently asked questions
Can kras, nras and braf tests in colorectal cancer be confirmed from symptoms alone?
No. Diagnosis combines history, examination and selected tests when indicated.
Does every patient need a procedure or operation?
No. Treatment depends on the confirmed diagnosis, severity, response and individual patient factors.
Which symptoms need urgent help?
A test appointment is not emergency care. Heavy bleeding, severe pain, fainting, fever, repeated vomiting or obstruction symptoms need prompt clinical assessment.