Why this topic matters
Rectal Bleeding: Piles or Cancer? is important because the same symptom can have several causes. Reliable information should help a patient decide between routine assessment and urgent care without encouraging self-diagnosis from a keyword, photograph or isolated symptom.
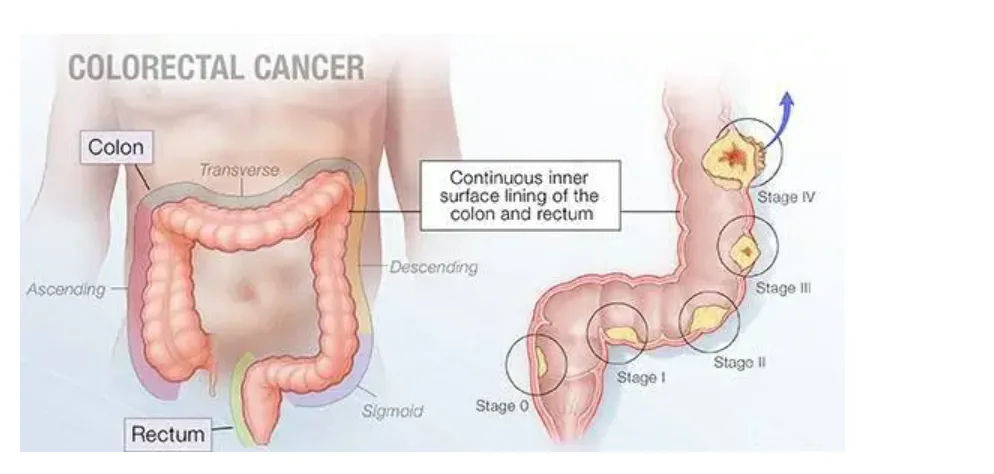
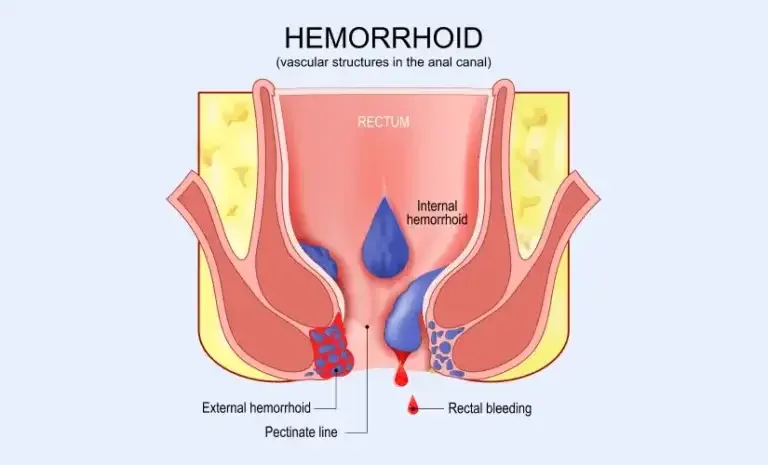
Piles are enlarged or displaced vascular cushions in the anal canal. They may cause painless bright-red bleeding, prolapse, itching or discomfort, but similar symptoms can also come from fissure, fistula, inflammation, polyps or cancer.
Treatment should match the haemorrhoid grade, dominant symptom, bowel habit and examination. A diagnosis of piles should not be used to dismiss persistent bleeding or warning signs without appropriate evaluation.
Symptoms and patterns to notice
The following patterns are not a diagnosis, but they provide useful information during assessment.
A key point is bright-red blood during or after a bowel movement.
Assessment considers a lump that comes out during stool and returns itself or needs manual reduction.
Treatment planning reviews itching, mucus or difficulty cleaning.
Follow-up pays attention to painful swelling when an external haemorrhoid becomes thrombosed.
A key point is symptoms made worse by constipation, straining or prolonged toilet sitting.
Warning signs that need prompt care
The severity and combination of warning signs matter.
A key point is large-volume bleeding, faintness or black stool.
Assessment considers severe anal pain with fever or spreading swelling.
Treatment planning reviews persistent bleeding with anaemia, weight loss or bowel habit change.
How clinicians assess the problem
Treatment should match the haemorrhoid grade, dominant symptom, bowel habit and examination. A diagnosis of piles should not be used to dismiss persistent bleeding or warning signs without appropriate evaluation. Before selecting a test, clinicians review duration, medicines, family history, previous procedures and overall health. The same investigation or treatment is not appropriate for every patient.
A key point is history of bleeding, prolapse, pain, medicines and bowel habit.
Assessment considers inspection and digital examination when tolerable.
Treatment planning reviews anoscopy or proctoscopy to assess internal haemorrhoids.
Follow-up pays attention to colonoscopy when age, anaemia, family history, bowel change or bleeding pattern raises concern.
Treatment and next steps
Care is stepped according to the confirmed diagnosis and severity.
A key point is fibre, adequate fluid, regular activity and avoiding straining.
Assessment considers short-term symptom relief and constipation treatment when appropriate.
Treatment planning reviews office procedures such as rubber-band ligation for selected internal haemorrhoids.
Follow-up pays attention to surgery for significant prolapse, recurrent bleeding, combined disease or failed conservative treatment.
A key point is soft stool and adequate pain relief are central after a procedure.
Assessment considers warm sitz baths and gentle hygiene may improve comfort.
Treatment planning reviews return to work depends on the procedure and the physical demands of the job.
Follow-up pays attention to heavy bleeding, fever, urinary retention or worsening pain needs prompt review.
Questions to ask at a consultation
Useful questions include: What is the most likely diagnosis? Which alternatives need exclusion? What will the test change? What may happen without treatment? How long is recovery, and which symptoms require urgent contact?
Instead of relying on unverified Best or Top claims, review qualifications, diagnostic reasoning, treatment explanation and follow-up systems.
Common misconceptions and safer decisions
One symptom cannot confirm piles (haemorrhoids). Bleeding colour, the type of pain or an internet image alone cannot reliably distinguish piles, fissure, fistula and cancer.
Temporary improvement does not prove that important disease is absent. Complete the planned assessment when anaemia, weight loss, family history or a persistent bowel change is present.
Unverified cure, guaranteed-success or Best and Top claims are not a substitute for clinical evidence. Understand the reason, expected benefit, alternatives, risks and follow-up before deciding.
Consider side effects, interactions and diagnostic delay before using laxatives, painkillers, antibiotics or herbal products for a prolonged period without clinical guidance.
Follow-up and everyday care
A key point is soft stool and adequate pain relief are central after a procedure.
Assessment considers warm sitz baths and gentle hygiene may improve comfort.
Treatment planning reviews return to work depends on the procedure and the physical demands of the job.
Follow-up pays attention to heavy bleeding, fever, urinary retention or worsening pain needs prompt review.
A short symptom diary recording pain, bleeding, stool frequency, medicine response and dietary changes can make patterns clearer at follow-up.
Persistent or progressive symptoms may need review even after an earlier normal report, while repeated unnecessary testing should also be avoided after an adequate negative evaluation.
Getting the most from a consultation
Before a consultation about piles (haemorrhoids), write down your three main concerns. Ask how the diagnosis will be confirmed, which tests are genuinely needed, what the realistic treatment goal is and which alternatives exist so the discussion stays focused.
Bring previous prescriptions, laboratory reports, colonoscopy, biopsy, CT or MRI reports and operation notes in date order. Reports from another hospital remain relevant because trends and earlier response may affect the current decision.
Diabetes, heart or kidney disease, pregnancy, blood thinners, allergies and tobacco use can change the safety of a procedure or medicine. Disclose them clearly and do not stop a prescribed medicine without advice from the prescriber.
At the end, repeat the diagnosis, next step, medicine dose, diet and activity advice, follow-up date and emergency warning signs in your own words. This simple check reduces misunderstandings and missed follow-up.
Treatment decision checklist
Before choosing treatment for piles (haemorrhoids), ask how certain the diagnosis is, how severe the current problem is and whether conservative care remains reasonable.
Compare each option by expected benefit, important risks, alternatives, recovery burden and its effect on future treatment choices. No procedure name alone establishes suitability.
Less pain, a smaller incision or a modern label may be useful features, but they are not the only decision factors when completeness, safety, function and recurrence are considered.
A second opinion can clarify major surgery, a permanent stoma, recurrent complex disease or reports that do not agree, but urgent treatment of bleeding, sepsis or obstruction should not be dangerously delayed.
Long-term monitoring and care coordination
After the immediate issue related to piles (haemorrhoids) is treated, review bowel habits, nutrition, medicines, family risk and any recommended surveillance.
Follow-up intervals are individual to diagnosis, pathology, procedure and recurrence risk. New bleeding, anaemia, weight loss, persistent pain or bowel-habit change should be reassessed rather than attributed automatically to an old diagnosis.
Colorectal care may involve gastroenterology, oncology, radiology, pathology, anaesthesia, stoma therapy, nutrition or a pelvic-floor team in addition to the surgeon.
Keep the primary coordinator, pending reports and the next decision point clear in the consultation or discharge plan so important results are not lost between services.
How to use this guide responsibly
This page synthesises information from linked medical authorities for patient education. It does not reproduce a source article and it is not a personalised prescription.
Medical evidence and guidance can change over time, so readers should check the review date and the linked authoritative source records.
The purpose is to support a better clinical conversation, not to encourage self-diagnosis, self-medication or selection of an operation from a marketing claim.
Emergency symptoms, rapid deterioration or a possible complication after recent surgery require help from the treating team or an emergency department rather than an online answer.
What good clinical care should include
Good clinical care starts with listening to the symptom history, performing a focused examination, explaining the working diagnosis and stating why each proposed test is relevant.
A treatment discussion should include reasonable alternatives, important risks, expected recovery and what may happen if treatment is deferred or declined.
When a report is pending, the patient should know who will review it, when the result will be communicated and which next step may change because of it.
Respect, privacy, informed consent, accessible communication and organised follow-up are part of patient safety just as much as technology and operative technique.
Clear records also help another clinician understand what has already been considered, reducing duplicated tests and contradictory advice during a second opinion or emergency visit.
Preparing for an appointment
Write down when symptoms started, bleeding colour and amount, timing of pain, bowel habit, weight change and family history. Bring prescriptions, colonoscopy, biopsy, CT or MRI, blood tests and operation notes.
A family member can help record important information and questions.
Key takeaways
Piles are enlarged or displaced vascular cushions in the anal canal. They may cause painless bright-red bleeding, prolapse, itching or discomfort, but similar symptoms can also come from fissure, fistula, inflammation, polyps or cancer. Timely diagnosis can reduce both unnecessary treatment and harmful delay. Emergency warning signs should not wait for a routine chamber appointment.
This article supports patient education and is not a personal diagnosis or prescription.
Frequently asked questions
Does every pile need an operation?
No. Many patients improve with bowel-habit correction or an office procedure. Surgery is selected for specific symptoms and grades.
Can bleeding be assumed to be piles?
No. Persistent or unexplained bleeding requires assessment because other colorectal conditions can present in the same way.
How can recurrence be reduced?
Maintaining soft stool, avoiding straining and following the recommended review plan can reduce symptom recurrence.