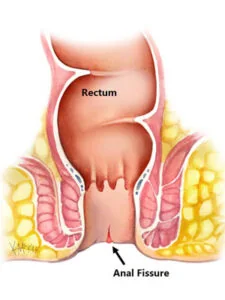
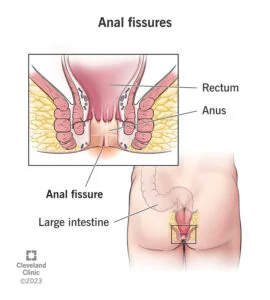
What is anal fissure?
An anal fissure is a small tear in the lining of the anal canal. It often follows passage of hard stool and causes sharp pain during a bowel movement, followed by burning or spasm that can last for minutes or hours.
A recent fissure may heal when stool is softened and pain-spasm is controlled. A chronic fissure can develop a skin tag, exposed sphincter fibres and persistent spasm. Atypical or multiple fissures require assessment for another disease.
An individual plan considers age, other illnesses, previous treatment and the effect of symptoms on daily life. General online information cannot replace an examination and report-based clinical decision.
Symptoms and warning signs
A key point is sharp cutting pain during stool.
Assessment considers burning pain or spasm after a bowel movement.
Treatment planning reviews a small amount of bright-red blood on tissue or stool.
Follow-up pays attention to fear of passing stool leading to more constipation.
A key point is a skin tag or recurrent split in chronic disease.
When to consult a colorectal specialist
Symptoms that resemble anal fissure may have another cause. Recurrent symptoms, interference with normal activity or failure to improve after treatment are reasons to review the diagnosis.
A key point is fever, pus or spreading swelling suggesting abscess.
Assessment considers heavy bleeding, black stool or dizziness.
Treatment planning reviews unusual lateral ulcers, multiple fissures, weight loss or chronic diarrhoea.
How the condition is diagnosed
No single test is appropriate for every patient. Selecting investigations from the history and examination reduces unnecessary testing while helping avoid a missed important diagnosis.
A key point is history of pain timing, bleeding and constipation.
Assessment considers gentle inspection, often sufficient to see a typical fissure.
Treatment planning reviews limited internal examination during severe pain.
Follow-up pays attention to further testing when the fissure is lateral, multiple, recurrent or associated with systemic symptoms.
Treatment options
Treatment aims to address the cause, severity, function and recurrence risk, using the least invasive effective option rather than focusing only on short-term symptom relief.
A key point is fibre, fluid and an appropriate stool-softening plan.
Assessment considers warm sitz baths and simple pain relief.
Treatment planning reviews prescription ointment to relax the internal sphincter in selected patients.
Follow-up pays attention to botulinum toxin or surgery when chronic symptoms do not respond to medical care.
When a procedure or surgery may be considered
A procedure is generally reserved for chronic fissure that remains symptomatic despite an adequate medical plan or when another finding changes the diagnosis. A patient should understand expected benefit, alternatives, recovery and material risks before giving informed consent.
A key point is prescription ointment to relax the internal sphincter in selected patients.
Assessment considers botulinum toxin or surgery when chronic symptoms do not respond to medical care.
Recovery after treatment or surgery
Recovery differs by procedure and patient. Following discharge advice on medicines, diet, activity and planned review helps identify complications early.
A key point is continue bowel-habit treatment after pain improves.
Assessment considers avoid repeated straining and prolonged toilet sitting.
Treatment planning reviews take prescribed ointment for the advised duration and discuss headache or dizziness.
Follow-up pays attention to return for review if bleeding persists or pain changes character.
Risks, recurrence and follow-up
No treatment is risk-free. Decisions compare the natural history of the condition, the limitations of non-operative care and the risks of a procedure.
A key point is constipation can reopen a healing fissure.
Assessment considers sphincter-relaxing treatments may have side effects and require individual selection.
Treatment planning reviews surgery is effective for selected chronic fissures but continence risk must be considered.
Making an informed treatment decision
A treatment plan for anal fissure should not depend on one test result alone. Symptoms, examination, disease severity, expected benefit, anaesthetic fitness, daily responsibilities and patient preferences all contribute to a sound decision.
Ask what the proposed procedure is intended to achieve, which alternatives exist, what may happen without treatment, the expected hospital stay, time away from work, and the important short- and long-term risks.
For cancer or complex recurrent disease, pathology, radiology, oncology and surgical opinions may change the sequence of care. Seeking a second opinion when uncertainty remains is a normal part of informed care.
When choosing a clinician or procedure, look for verified qualifications, relevant training, a clear diagnosis, documented consent and an organised follow-up system rather than unverified Best, Top or guaranteed-cure claims.
Long-term care and common misconceptions
Improvement in symptoms from anal fissure does not always prove that the underlying condition has completely resolved. Complete the prescribed course, review pathology or imaging results, and attend planned follow-up.
Food, fluid, activity and bowel habits can support recovery in many colorectal conditions, but lifestyle advice is not definitive treatment for confirmed cancer, abscess, obstruction or another structural disease.
Unverified internet remedies, unknown herbal products or prolonged self-directed antibiotics can hide bleeding, cause side effects or delay the correct diagnosis. Tell the clinician about every medicine and supplement used.
Seek reassessment when pain, bleeding, fever, weight loss or bowel change is new or different from the previous pattern instead of assuming that an old diagnosis still explains it.
What to confirm at follow-up
At follow-up for anal fissure, confirm whether the diagnosis or stage has changed, whether response is as expected, and whether a new report alters the plan. Describe specific changes in pain, bleeding, discharge, fever, appetite, weight and bowel habit rather than only saying that you feel better.
Write down how long each medicine should continue, which side effects are expected, when to stop and call, and how to maintain bowel habits after the prescription ends. Do not change the dose of a similarly named medicine without checking.
After a procedure or surgery, wound, pathology, stoma, continence, diet, activity and return-to-work plans may differ. Confirm the date of the next visit, test or dressing and know how to seek urgent advice.
If symptoms return, reassess recurrence, a new complication or a different diagnosis rather than restarting an old treatment without review. Keeping reports and operation notes makes future assessment safer and more efficient.
Preparing for an appointment
Bring previous prescriptions, test reports, operation notes, allergies and a current medicine list. Note when symptoms began, what worsens them and how often bleeding or discharge occurs.
Do not wait for a routine appointment when emergency symptoms are present; seek prompt assessment at the nearest emergency department.
 Anal Fissure Treatment
Patient education visual
Anal Fissure Treatment
Patient education visual